Hiroshima, Japan







On August 6, 1945, the U.S. detonated the atomic bomb “Little Boy” over the city of Hiroshima. Of the 350,000 citizens, about 140,000 had died by the end of the year. The surviving “Hibakusha” suffered from the late effects of radiation, including increased incidence of cancer.
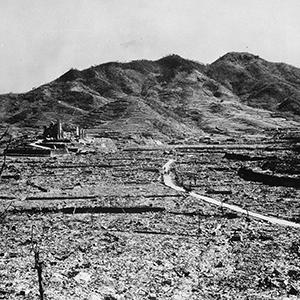
Photo: The view over Hiroshima from the Red Cross Hospital in 1945. The nuclear detonation released huge amounts of energy, 50 % of which leveled the inner city in the form of a massive pressure wave, demolishing almost all buildings within a 2 km radius. Credit: U.S. Government / public domain
History
During World War II, the U.S. produced three nuclear bombs. After the successful Trinity Test on July 16, 1945, the U.S. detonated the remaining two bombs over Japanese cities. A uranium bomb called “Little Boy,” was dropped on Hiroshima on August 6, 1945, a plutonium bomb called “Fat Man,” on Nagasaki on August 9. In Hiroshima, the T-shaped Aioi Bridge, in a populated commercial and residential area, was selected as the target. The bomb detonated at an altitude of 580 m with an explosive force equivalent to about 15,000 tons of TNT.
Health and environmental effects
The nuclear detonation released enormous amounts of energy, roughly 50 % of which was blast energy. The pressure wave caused by the explosion demolished almost all buildings within a 2 km radius around the hypocenter, including the major hospitals. Ear-drums and lungs burst even at a distance of several kilometers, while the wind reached velocities comparable to large hurricanes and parts of buildings. Vehicles and dead bodies hurtled as deadly projectiles through the ravaged streets.
About 35 % of the energy was released in the form of heat and led to a giant fire storm, which quickly engulfed the entire inner city. Most buildings within a radius of two kilometers fell victim to the flames. With temperatures of up to 3,000–4,000 °C around the hypocenter, all living things burned to ashes and only “nuclear shadows” remained on the pavement. Uncovered skin burned within a radius of 3.5 km. People hiding in bunkers or cellars died from carbon monoxide poisoning or suffocation. The remaining 15 % of the total energy was released in form of radioactivity.
From a total of 298 medical doctors, only 28 survived the nuclear explosion. Together with about 130 nurses and 28 pharmacists, they were the only ones able to provide first aid to the survivors. Most of the deaths in the first two weeks occurred due to burns, external injuries and acute radiation exposure. From the third to the eighth week, people exposed to more than 3 Sievert (Sv) of radiation died from organ failure, bloody diarrhea and vomiting or bone marrow depression with anemia, immunodeficiency and bleedings. According to conservative estimates, at least 45,000 people died on the first day after the bombing. By the end of 1945, this number had risen to about 140,000. The exact number of casualties will never be known, however, because it is not known how many people were staying in the city during the final days of the war. Also, documents were lost in the flames; whole families perished, leaving no one to account for missing relatives; and the entire social system collapsed after the nuclear bombing, further complicating mortality assessments.
The first long-term effects of external radiation to be observed were keloid scars and cataracts. Starting in 1947, a non-linear increase of leukemia was noted. Leukemia incidence peaked in the first half of the 1950s and gradually declined after that. The relative risk of leukemia is presumed to be about 16 times higher for people who received 2–3 Sv of radiation as compared to the general population. Until today, leukemia incidence in Hiroshima is slightly higher than in the rest of Japan.
On the other hand, the incidence of solid tumors is continually increasing as survivors are getting older, as is the incidence of myelodysplastic syndrome. While at first mainly thyroid cancer showed a rising incidence, cancers of the breast, stomach, large intestines, skin, liver, gallbladder, ovary and urinary bladder soon followed. The epidemiological Life Span Study (LSS), begun in 1950, showed that the incidence of cancer was proportional to the radiation exposure dose. Also, the incidence of cancer was higher in people exposed at younger age. According to the LSS, the estimated risk of solid cancers is about 1.5 times higher in the survivors of the bombing than in the general population.
Besides cancer, other diseases with higher incidence in the survivors cohort were benign tumors, endocrine disorders, hypertension and stroke, as well as heart and liver disease. Since the frequency of chromosomal aberrations was shown to increase with radiation dose, it can be used as a “biological dosimeter.” In case of intrauterine exposure, increases in microcephaly and mental retardation were noticed in offspring of survivors.
Outlook
The Japanese term for the survivors of the nuclear bombings is “Hibakusha.” Most of the Hibakusha still alive today were exposed to radiation at a very early age so that detrimental long-term effects and increased morbidity rates can still be expected to occur in this population. But much is still unknown. The effects of internal radiation from nuclear fallout were not accounted for in the LSS, for example. Also, because the study was only begun in the year 1950, radiogenic effects of the first five years after the bombing, especially those pertaining to perinatal morbidity and mortality, were never properly assessed. Finally, some Hibakusha groups are accusing the government of covering up the health effects of radiation on future generations for political reasons.
References
- Shigematsu I. “A-bomb Radiation Effects Digest.” Bunkodo, Tokyo, 1993.
- Kamada N. “One Day in Hiroshima – An Oral History.” Japanese affiliate of IPPNW, 2007. www.ippnw.org/pdf/book-one-day-in-hiroshima.pdf
- Matsuzaka Y. “Hiroshima Genbaku Iryoshi (Medical care history of the atomic bombed population of Hiroshima).” Hiroshima, 1961
- “A Brief Description.” Radiation Effects Research Foundation (RERF), Hiroshima, June 2013. www.rerf.jp/shared/briefdescript/briefdescript.pdf
- Pierce DA. “Studies of the mortality of atomic bomb survivors: 1950-1990.” Radiation Res 146, 1-27, 1996. www.ncbi.nlm.nih.gov/pubmed/8677290
- Ohkita T. “Acute medical consequences of Hiroshima and Nagasaki.” in “Last Aid.” IPPNW 1985.